1. Vaccine Passports ignore the naturally immune.
– Natural immunity is durable and long lasting to the point that if you’ve had COVID-19 you will probably make antibodies for a lifetime. A study out of Israel states that “after adjusting for comorbidities, we found a 27.02-fold risk (95% CI, 12.7 to 57.5) for symptomatic breakthrough infection as opposed to symptomatic reinfection.” The NIH highlights natural immunity while stating they hope that vaccine induced immunity will be similar. Another pre-print out of Israel shows both natural and vaccine immunity to be strong with natural immunity being more protective. This study in Cell as highlights that “broad and effective immunity may persist long-term in recovered COVID-19 patients.”
– In fact the FDA will only collect blood from the previously naturally infected (not from the vaccinated) “to ensure that COVID-19 convalescent plasma collected from donors contains antibodies directly related to their immune responses to SARS-CoV2 infection…”
– The practice of requiring the previously infected to be vaccinated is inconsistent with past CDC policy as after the H1N1 flu the CDC stated: “If you have had 2009 H1N1 flu, as confirmed by an RT-PCR test, you should have some immunity against 2009 H1N1 flu and can choose not to get the 2009 H1N1 vaccine.”
– A recent study out of the Cleveland Clinic Health System found that “not one of the 1359 previously infected subjects who remained unvaccinated had a SARS-CoV-2 infection” and concluded that “individuals who have had SARS-CoV-2 infection are unlikely to benefit from COVID-19 vaccination.”
2. It is hard to tell who is naturally immune.
– An estimated 15% of all COVID-19 infections (18.4 million) are considered asymptomatic by the CDC. Antibody test can uncover some of these naturally immune, but not all. Many recovered individuals have robust anamnestic immune responses without detectable antibodies to viruses such as Hepatitis B and SARS-CoV-2 (for both memory B cells and memory T cells).
– These asymptomatic individuals were essentially immune without prior exposure to SARS-CoV-2. The results of this pre-print indicate that in some people, exposure to SARSCoV2 elicits an innate and T-cell immune response, leading to an abortive infection, without development of antibodies (seroconversion). Our current understanding of the immune system does not fully understand this phenomenon hence it is impossible to determine which unexposed individuals have pre-existing immunity.
– Pre-existing T-cell immunity may not always provide simple immunity, but may offer natural protection against severe disease. This protection due to cross-reactive immunity may contribute to a milder course of COVID-19 by limiting viral propagation.
3. Vaccine Protection Against Infection/Transmission Wanes Rapidly.
As infection rates among the vaccinated rival those of the unvaccianted it seems clear that the vaccines do not stop infection and transmission. Vaccine passports and mandated are untenable for a vaccine that does not stop transmission (lacking sterilizing immunity).
Furthermore, each vaccines varies in its ability to stop transmission. A recent study on the Pfizer vaccine concluded that “BNT162b2-induced protection against infection appears to wane rapidly after its peak right after the second dose…” Will we provide one passport to all vaccine recipients even though they pose varying risk of transmission?
Finally, healthy people carry many viruses and do not spread them, in the case of the flu asymptomatic carriage was as high as 35%.
4. Do Vaccine Passports Keep Us Safer?
– The simple answer to this is marginally, if at all. Vinay Prasad, MD, MPH says it best in that “a vaccine passport results in a trade-off. It very modestly changes the risk to vaccinated individuals and those who do not have a vaccine option.” There are multiple reasons for this:
a. Protection: The belief is that those that are vaccinated are protected from severe disease.
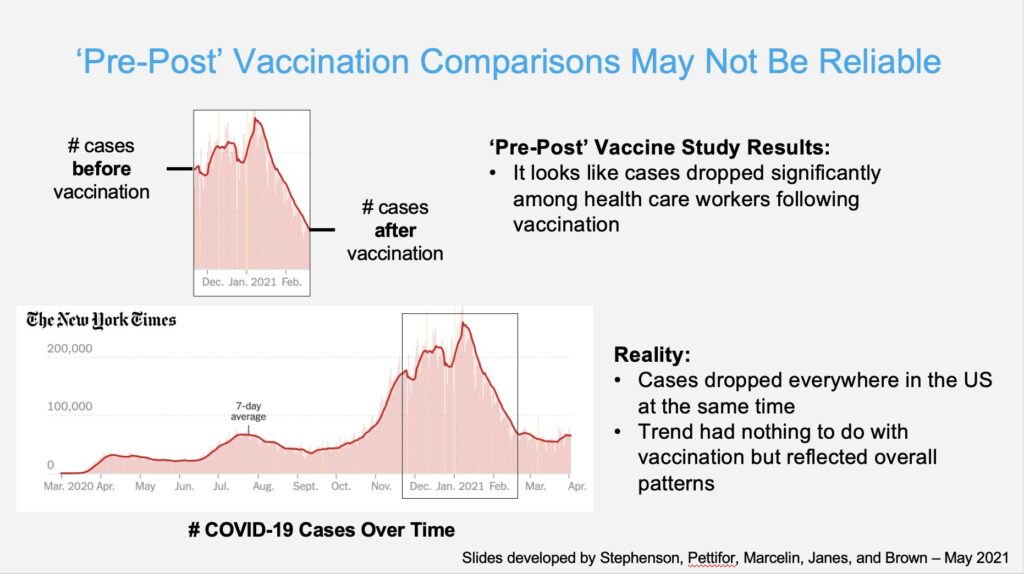
b. Prevalence: Prevalence of circulating virus needs to be included in any risk assessment. As the diagram below shows the cases of COVID-19 in the vaccinated dropped, but was that due to the vaccine or simply correlated with the overall drop of cases in the US?
c. Risk Reduction: When looking at risk it is important to examine both the relative risk reduction (RRR) and absolute risk reduction (ARR) as highlighted recently in the Lancet: “Ranking by reported efficacy gives RRR of 95% for the Pfizer, 94% for the Moderna, 90% for the Gamaleya, 67% for the J&J, and 67% for the AstraZeneca vaccines. However, RRR should be seen against the background risk of being infected and becoming ill with COVID-19, which varies between populations and over time. Although the RRR considers only participants who could benefit from the vaccine, the ARR, which is the difference between attack rates with and without a vaccine, considers the whole population. ARRs tend to be ignored because they give a much less impressive effect size than RRRs: 1.3% for the AstraZeneca, 1.2% for the Moderna, 1.2% for the J&J, 0.93% for the Gamaleya, and 0.84% for the Pfizer vaccines. In the context of the clinical trials against SARS-CoV-2, the vaccines do very little to reduce absolute risk.
5. Vaccine Passports segregate society.
A recent BJM opinion piece explained, “ultimately, we need to facilitate the economic growth of emerging economies to increase the health, wellbeing, and security of all. Vaccine passports interfere with that future as they create a structural barrier to sustainable development, benefiting only the few at the expense of so many.”
6. Vaccine Passports threaten privacy.
– The ACLU, while not opposed to vaccine passports in principal, has significant concerns with a digital vaccine passport system. They state it must be primarily paper-based with an optional digital component, decentralized and open source, not allow for tracking or the creation of new databases, and not encourage overuse, turning us into a checkpoint society.
7. Vaccine Passports raise legal and logistic issues.
– Stefan Baral (MD.MPH) of Public Health at Johns Hopkins detailed logistical concerns such as who will ask for it, how will they check it, where will this occur.